A Surgeon’s Perspective on Modern Vision Correction
Implantable Contact Lenses (ICL) represent one of the most advanced forms of refractive vision correction available today. Unlike lens replacement surgery, ICL does not remove the natural lens of the eye. Instead, it adds a highly precise optical element inside the eye to correct refractive error while preserving natural anatomy.
For patients with moderate to high myopia, astigmatism, thin corneas, or those unsuitable for laser eye surgery, ICL can offer exceptional clarity and long-term stability.
Two of the most common questions patients ask are:
- Are Implantable Contact Lenses safe?
- How long do they last?
From a surgical standpoint, modern ICL technology has demonstrated strong safety data and long-term performance when used in appropriately selected patients.
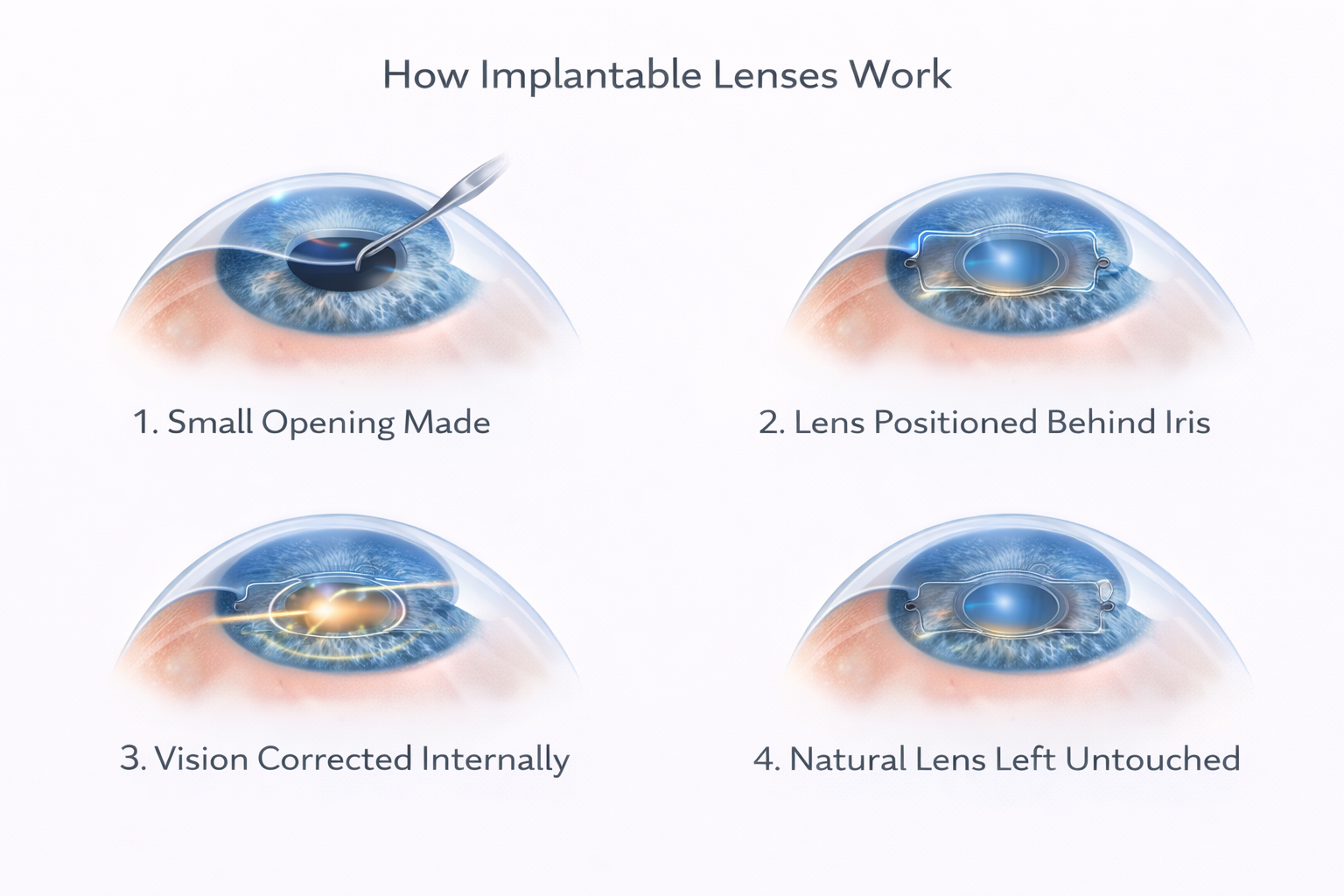
What Exactly Is an Implantable Contact Lens?
An Implantable Contact Lens is a thin, flexible, biocompatible lens placed behind the iris and in front of the natural lens.
The natural crystalline lens remains in place. Nothing is removed.
This is why ICL is referred to as phakic intraocular lens surgery, the eye retains its natural focusing lens.
Unlike laser eye surgery, which reshapes the cornea, ICL works by adding optical power inside the eye. The result is highly precise correction without altering corneal structure.
Because the cornea is untouched, ICL is particularly valuable for:
- Higher prescriptions
- Thin corneas
- Irregular corneal shape
- Patients unsuitable for laser procedures
The procedure is additive, reversible, and structurally conservative.
Are Implantable Contact Lenses Safe?
Modern ICL technology has been used for over two decades and has undergone continuous refinement.
Current-generation ICL lenses are made from a specialised collagen-based biocompatible material that integrates safely within the eye. The lens design includes a central port that allows natural fluid circulation, maintaining healthy intraocular pressure and normal physiology.
From a surgical perspective, safety depends on several key factors:
1. Precise Measurement and Sizing
The lens must be accurately sized to the patient’s anterior chamber depth and eye anatomy. Advanced imaging technology is essential.
2. Correct Patient Selection
ICL is not suitable for every patient. Detailed diagnostic assessment determines eligibility.
3. Modern Surgical Technique
The lens is inserted through a very small incision, typically self-sealing and stitch-free. When these factors are respected, complication rates are low and outcomes are highly predictable. Like any intraocular procedure, ICL surgery carries risks, including infection, pressure changes, or lens-related complications, but in well-selected candidates these risks are uncommon.
How Long Do Implantable Contact Lenses Last?
Implantable Contact Lenses are engineered for long-term performance inside the eye. The material used in modern ICL technology is highly biocomatible and designed to remain stable for decades without degrading, dissolving, or losing optical quality. Unlike external contact lenses, which are subject to daily wear, surface deposits, and gradual replacement, an implantable lens becomes part of the internal optical system of the eye. Once positioned correctly, it functions continuously and consistently, unaffected by tear film instability, environmental exposure, or daily handling.
Because the lens sits behind the iris and in front of the natural crystalline lens, it operates in a protected anatomical space. Patients do not need to remove it, clean it, replace it, or manage any maintenance routine. The correction remains stable throughout the day and over the years, offering a level of consistency that surface-based correction cannot match.
One of the key advantages of ICL technology is that it preserves the natural lens of the eye. This means that the procedure is additive rather than destructive. If visual needs change in the future, the lens can be removed or exchanged. For example, if a patient later develops cataracts as part of the normal aging process, the ICL can be safely removed at the time of cataract surgery, and a new intraocular lens can be implanted. In this sense, ICL does not limit future options, it keeps them open.
Looking ahead, implantable lens technology continues to evolve. Future upgrades are likely to focus on even greater optical precision, enhanced material science, and expanded customisation. We are already seeing improvements in lens sizing algorithms, anterior chamber imaging, and optical modelling, which allow surgeons to tailor lens selection with remarkable accuracy. Advances in wavefront-guided diagnostics may further refine how we correct subtle higher-order aberrations, potentially improving night vision and contrast sensitivity.
There is also ongoing development in adjustable and light-responsive intraocular technologies, which may one day integrate with phakic lens platforms. While current ICL designs provide stable, fixed correction, future generations may incorporate enhanced micro-optical refinements or improved vault dynamics to optimise long-term compatibility and visual performance.
Importantly, because ICL preserves the natural lens, patients who undergo the procedure are not closing the door to future innovations. If more advanced refractive solutions emerge decades later, the implantable lens can be exchanged as part of a carefully planned surgical strategy. This flexibility is one of the reasons many surgeons view ICL not simply as a solution for today, but as a structurally conservative option that protects tomorrow’s choices.
From a surgical perspective, that balance between long-term stability and future adaptability is what makes modern implantable contact lenses such a powerful component of contemporary refractive practice.
Will ICL Need Replacing in the Future?
ICL does not require routine replacement.
However, it is important to understand one key distinction: ICL corrects refractive error, but it does not prevent natural ageing of the eye.
As patients reach their mid-40s and beyond, presbyopia develops due to aging of the natural lens. Later in life, cataracts may form as part of normal biological aging. If cataract surgery becomes necessary decades later, the natural lens is removed at that stage, and the ICL is typically removed during the procedure. This is not a failure of the ICL, it is simply the natural progression of the eye over time.
Is Vision Stable Long-Term?
One of the strongest advantages of ICL is stability.
Because the lens sits inside the eye:
- It does not depend on tear film
- It does not dry out
- It does not shift with blinking
- It does not reshape corneal tissue.
Patients frequently report that their vision feels:
- Sharper
- More consistent
- More stable throughout the day.
For high prescriptions especially, visual quality can be superior to glasses or surface contact lenses.
Who Is Most Suitable for ICL?
Implantable Contact Lenses are most commonly recommended for patients with moderate to high myopia, significant astigmatism (when toric designs are used), thin corneas, or those who are unsuitable for laser eye surgery due to corneal thickness or shape. They are also particularly valuable for patients who experience dryness or intolerance with surface contact lenses and want a long-term solution that does not rely on daily handling. Because the natural lens of the eye is preserved, ICL offers a reversible and structurally conservative form of vision correction.
However, suitability is strongly influenced by age and the natural changes that occur inside the eye over time.
Ages 20–39: The Ideal ICL Candidate
Patients in their twenties and thirties are typically the strongest candidates for Implantable Contact Lenses. At this stage, the natural crystalline lens remains clear and flexible, and presbyopia has not yet developed. For individuals with stable moderate to high myopia or astigmatism, ICL provides precise correction without altering the cornea.
This age group often includes professionals, active individuals, and long-term contact lens wearers seeking freedom from glasses or surface lenses. Because the natural lens is still functioning normally, preserving it is advantageous. ICL corrects refractive error while maintaining the eye’s natural accommodation and structure.
From a surgical perspective, this is the phase where additive correction makes the most sense. The eye is healthy, the prescription is stable, and the patient benefits from long-term clarity without committing to lens replacement.
Ages 40–50+: The Transitional Phase
In the forties, the eye begins to undergo a natural change known as presbyopia. The natural lens gradually loses its flexibility, making near vision more difficult. While ICL can still correct distance refractive error in this age group, it does not prevent or reverse presbyopia because the natural lens remains in place.
For patients in their early forties who still have a clear natural lens and primarily wish to correct distance vision, ICL can remain an excellent option. However, they must understand that reading glasses may still be required as near focus declines.
As patients approach their late forties and early fifties, surgical planning becomes more nuanced. If early lens dysfunction or cataract development is present, refractive lens exchange or advanced intraocular lens implantation may provide a more comprehensive long-term solution. In these cases, removing the ageing natural lens and replacing it with multifocal or trifocal technology can address both distance and near vision simultaneously.
The decision in this age range depends heavily on lens clarity, lifestyle demands, and visual priorities.
Ages 70+: Cataract and Lens-Based Solutions
In patients over seventy, ICL is rarely appropriate. By this stage, most individuals will have some degree of cataract formation or age-related lens opacity. Because ICL preserves the natural lens, implanting it in the presence of cataract would not address the underlying problem.
Instead, cataract surgery with intraocular lens implantation becomes the preferred treatment pathway. Modern monofocal, multifocal, trifocal, or adjustable intraocular lenses can restore clarity while also addressing presbyopia and refractive error.
At this stage of life, the goal shifts from additive correction to replacement of the ageing lens altogether. Ultimately, suitability for Implantable Contact Lenses is determined through detailed diagnostic imaging, including anterior chamber depth measurement, corneal assessment, and evaluation of lens clarity. Age is not the only deciding factor, but it plays a central role in selecting the most appropriate long-term strategy.
From a surgical standpoint, the key is matching the procedure to the biological stage of the eye, preserving the natural lens when it is healthy, and replacing it when it is no longer functioning optimally.
ICL vs Lens Replacement by Age Range
A practical guide to the most common treatment pathway by age. Final suitability is always confirmed by diagnostics and surgeon assessment.
Age range
ICL (Phakic Lens)
Lens Replacement (RLE / Cataract IOL)
Clinical note: Final recommendations depend on diagnostics such as anterior chamber depth, corneal health, lens clarity, endothelial cell status, and the patient’s visual goals.
ICL vs Lens Replacement: Understanding the Difference
This distinction is essential.
ICL (Phakic Lens Surgery)
- Natural lens remains
- Additive procedure
- Typically for younger patients
- 可逆
- Corrects refractive error.
Lens Replacement (Cataract / Refractive Lens Exchange)
- Natural lens removed
- Intraocular lens implanted
- Often for presbyopia or cataract
- Permanent change
- Can restore near and distance vision with multifocal/trifocal technology.
They are different procedures designed for different patient profiles.
Real-World Outcomes in London
Case Study: Sarah, 56 Architect, Toric ICL
Sarah had high myopia and astigmatism. She was not suitable for laser due to corneal characteristics. A toric Implantable Contact Lens was selected to correct both refractive error and astigmatism.
Post-operatively, she described her vision as sharper and more stable than with glasses. Her precision work as an architect became easier, particularly when reviewing fine drawings.
This reflects one of the key strengths of toric ICL; precise, stable astigmatic correction without altering the cornea.
A Modern Long-Term Solution
From a surgical perspective, ICL remains one of the most elegant solutions for refractive correction in suitable candidates.
- It preserves the natural lens.
- It preserves corneal structure.
- It delivers high optical precision.
- It remains stable long-term.
- It is reversible if required.
For patients who are not ideal candidates for laser surgery, or who seek high-definition clarity without removing the natural lens, Implantable Contact Lenses represent a safe and sophisticated option.
The key, as always, is careful assessment, precise measurement, and selecting the right procedure for the right patient.
That is where experience and technology truly matter.
Choosing the Right Clinic and Lens Technology Matters
As a surgeon, one of the most important decisions we make is not simply how to perform the procedure, but which lens to implant and why. Implantable lenses are designed to remain inside the eye for decades, becoming part of the patient’s visual system. For that reason, precision in measurement and lens selection is absolutely critical. Even small differences in eye structure, corneal shape, or visual demands can influence which lens will provide the most stable and natural outcome.
Not all implantable lenses are the same, and not all patients benefit from the same optical design. Some patients require toric lenses to correct astigmatism, while others benefit from trifocal technology to restore functional vision across multiple distances. The key is understanding not only the measurements of the eye, but how the patient uses their vision in daily life! Whether that involves working on screens, driving at night, or maintaining visual independence without glasses.
At specialised centres such as EuroEyes, we use advanced diagnostic imaging to assess the eye in exceptional detail before recommending treatment. This allows us to select lens technology that aligns precisely with the patient’s anatomy and visual goals. From a surgical standpoint, this level of planning is what allows us to achieve consistent, predictable outcomes and provide patients with vision that feels clear, stable, and natural long after the procedure.
Implantable lens surgery is not simply about correcting a prescription. It is about restoring confidence in vision, and that begins with choosing the right lens, in the right eye, for the right patient.


